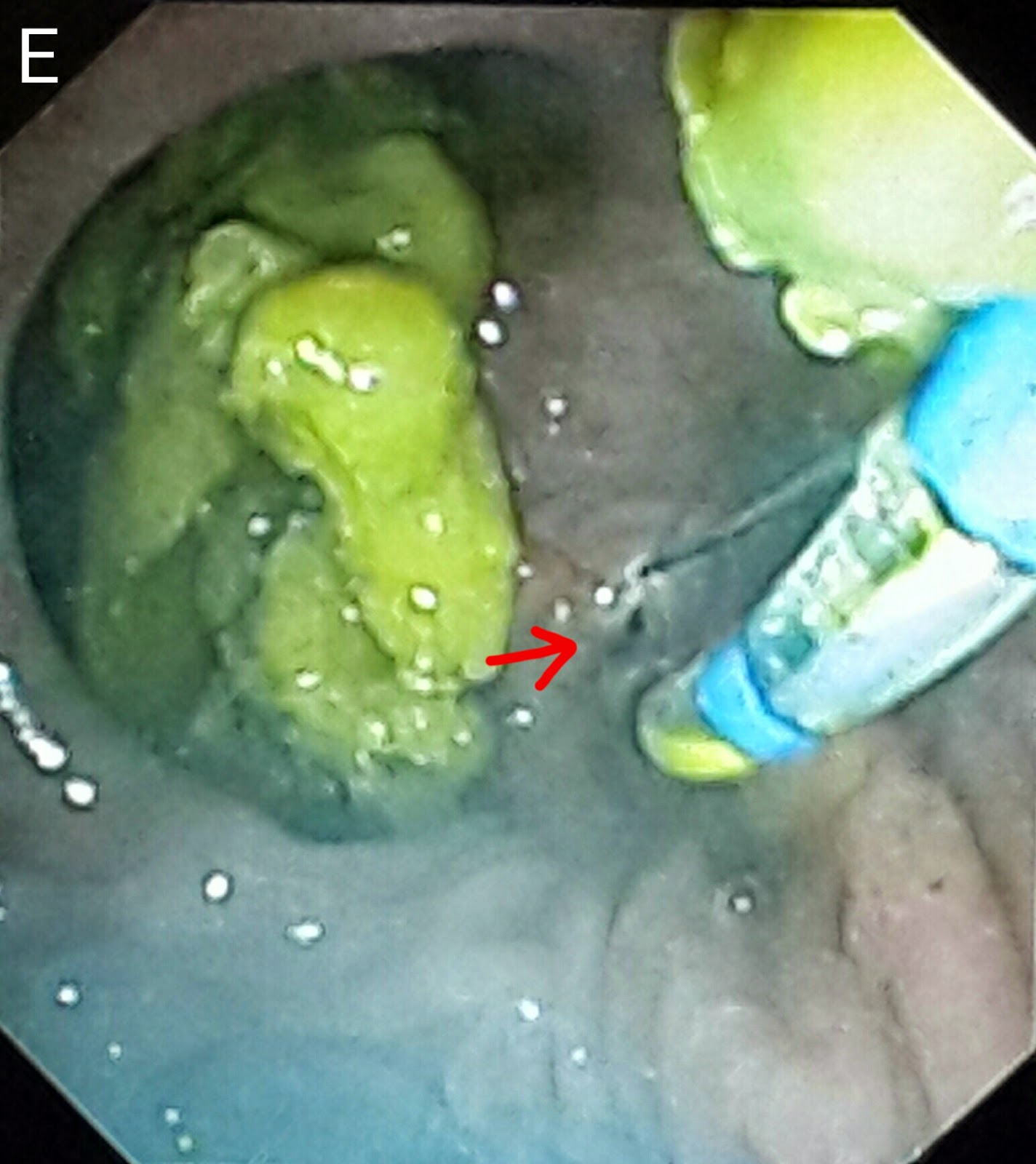
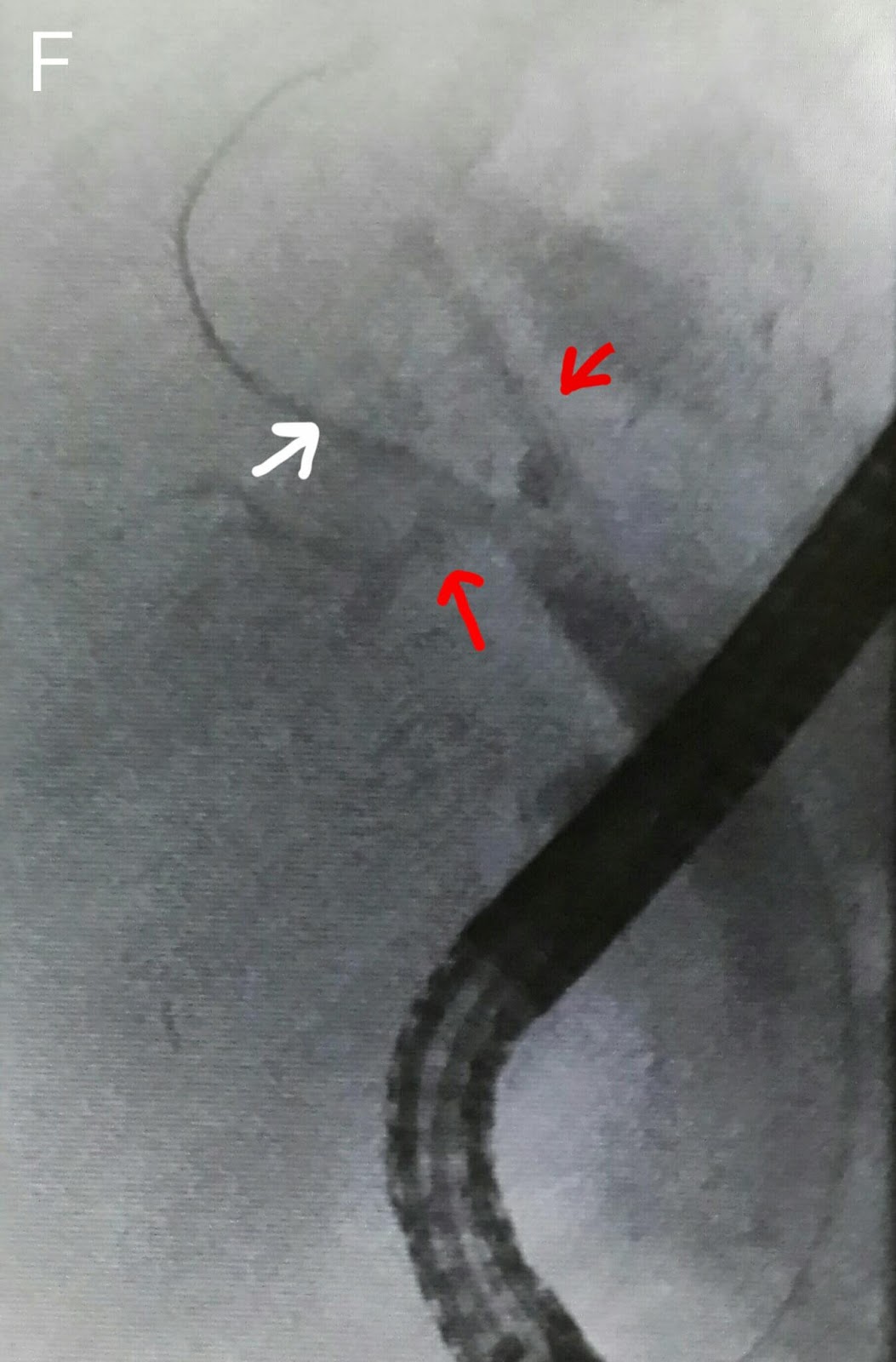
This 40 year old gentleman is an old patient of ours. He has been treated for hepatitis C and extra hepatic portal venous obstruction. He has been regularlyundergoing ERCPs at our center for bile duct obstruction. We usually clear the CBD and place a new plastic stent at each visit. This time around we couldn't see the previously placed stent and suspected that it had migrated into the bile duct. This was confirmed on flouroscopy (A: black arrows). We first attempted to pull the stent out using a stone extraction basket (B: white arrows show the stent. Black arrows mark the basket). This was unsuccessful so our next maneuver was to thread the stent with a guidewire (C: white arrows show the stent and black arrows mark the guidewire). The wire was passed to thread a Soehendra stent retriever over it (D: white arrow). The stent was properly engaged (E: white arrow indicates the stent retriever and black arrow market the engaged lower end of the stent). The old stent was then pulled out (F: black arrow shows the friable sludge ridden end of the stent being pulled by the Soehendra stent retriever-white arrow). We could have directly pulled free stent out through the scope channel but were concerned that it might break since the distal end was very cracked and friable. We used a snare to pull it out (G: white arrow shows the snare. H: The retrieved stent l. A wide papillotomy was done (I: white arrow). The CBD was swept with a stone extraction balloon (J: black arrow shows the inflated balloon in the bile duct). A lot of debris was removed (K: white arrows). Finally a 10 French diameter plastic stent of 12 cm length was placed (L: black arrows). This was a stent with a curved proximal end. Not the the classical pigtail shape. This would help in retention of the stent keeping in mind the papillotomy.