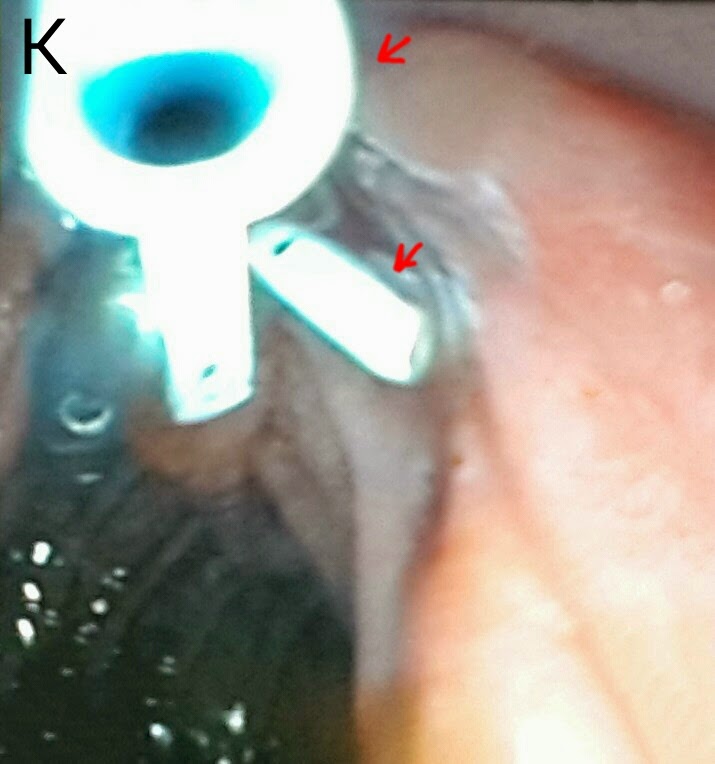
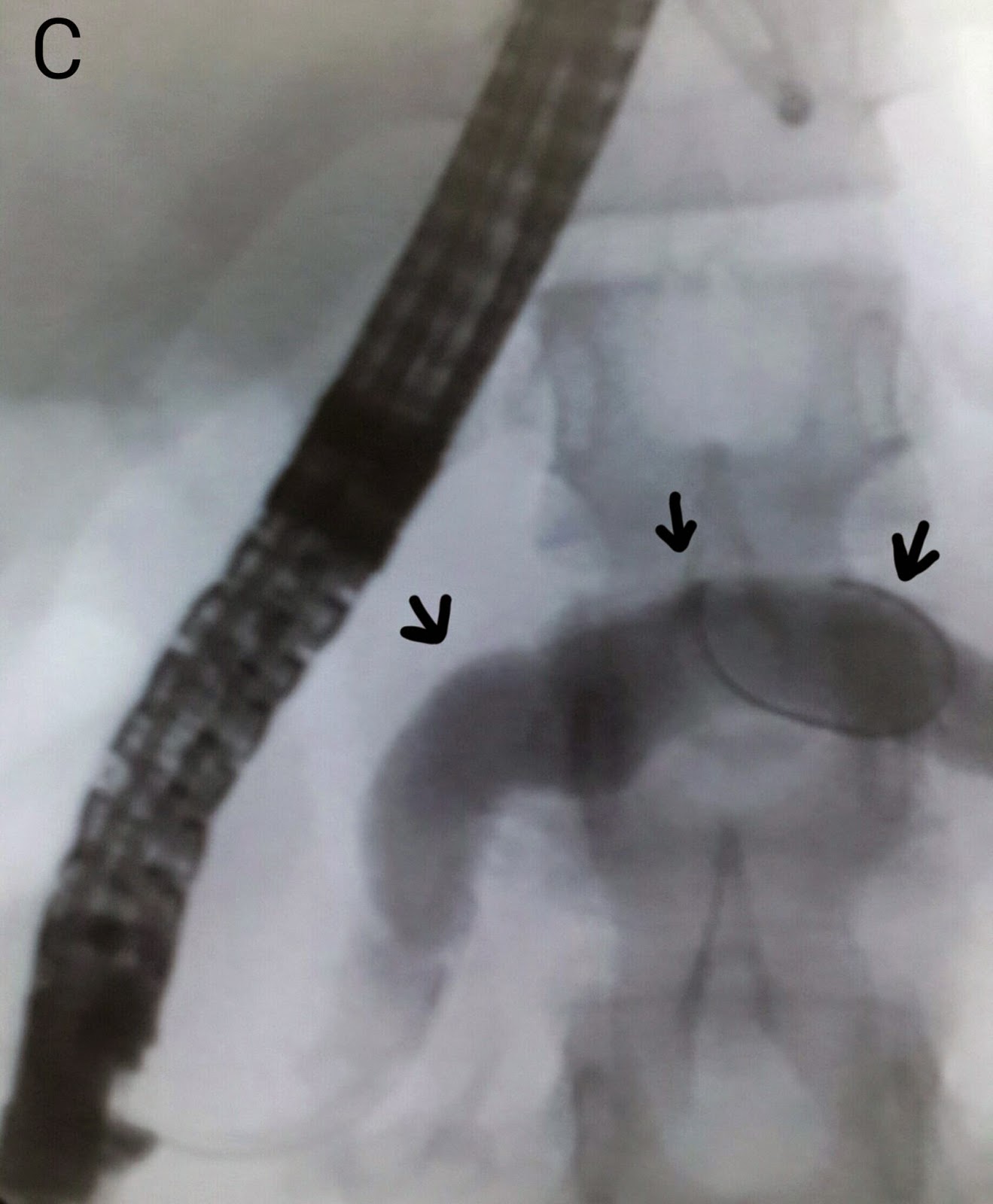
This gentleman had recently undergone a live related liver transplant. His bilirubin levels started to rise along with his alkaline phosphatase. An anastomotic stricture was suspected and confirmed on MRCP (A: red arrow shows the strictured area along the left maim duct). A guidewire was passed into the left system (B: black arrows mark the guidewire in the left ductal system). A TTS stricture dilatation balloon was manoeuvred across the affected segment and inflated to 9mm (C: black arrows indicate the balloon in the stricture site. The balloon isn't clearly visible because we haven't mixed any contrast with the saline). Repeat contrast injection some improvement in ductal filling (D). We then placed a plastic stent of 10 French diameter and 12 cm length (E: black arrows mark the deployed stent).