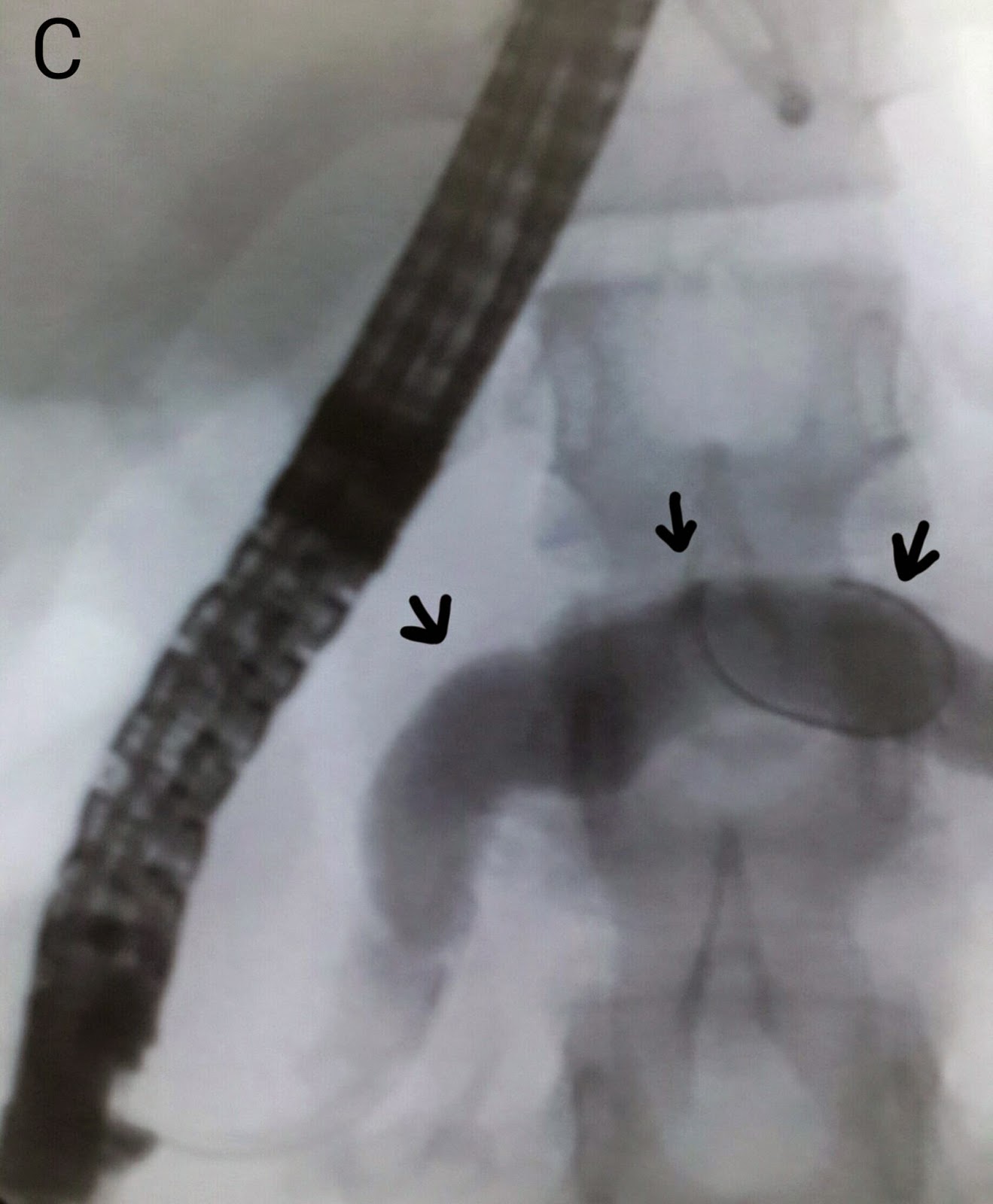
This 13 year old girl was first seen by us over a year ago in June last year (The case was posted on the blog in August) http://ercp365.blogspot.com/2013/08/pancreatic-duct-calculi.html. She had been having recurrent episodes of pancreatitis. Her ERCP showed multiple pancreatic duct stones (A: white arrows) and a diagnosis of pancreatic divisum as the cause of pancreatitis was made. At that time, looking at the number of stones in the pancreatic duct, we had referred this patient for surgery. The patient's family seemed reluctant for any surgery however and turned up at our outpatient again after over a year in which she had undergone an ERCP at another centre as well (No attempts were made at stone extraction in that attempt either). We again tried to convince the family for surgery but they didn't seem willing. She was put on list again and this time around we went in first via the accessory papilla (B: white arrow indicates the accessory papilla and black arrow marks the major papilla). Contrast injection outlined a grossly dilated pancreatic duct without any negative shadows (C: black arrows show the pancreatic duct). We did a wide papillotomy at the accessory papilla (D). The inner tissue was obviously not what we normally see and showed the degree of fibrosis secondary to chronic repeated inflammation (E: black arrow). A stone extraction balloon assembly was manoeuvred into the pancreatic duct (F: black arrow). The pancreatic duct was swept with the balloon (G: white arrow), which didn't result in extrusion of any debris. This was followed by an occlusion pancreaticogram (H: white arrow shows the inflated balloon and black arrows show a clear dilated pancreatic duct free of stones). The guidewire was withdrawn and then reinserted, this time via the major papilla and into the common bile duct (I: black arrows). We ended the procedure with a cholangiogram which outlined a clear CBD (J: black arrows). Retrospectively, it is possible that the stones seen the first time around in the pancreatic duct were actually aggregations of debris and this had cleared over the past year. In any case we hope she fares well and is able to avoid surgery.













No comments:
Post a Comment