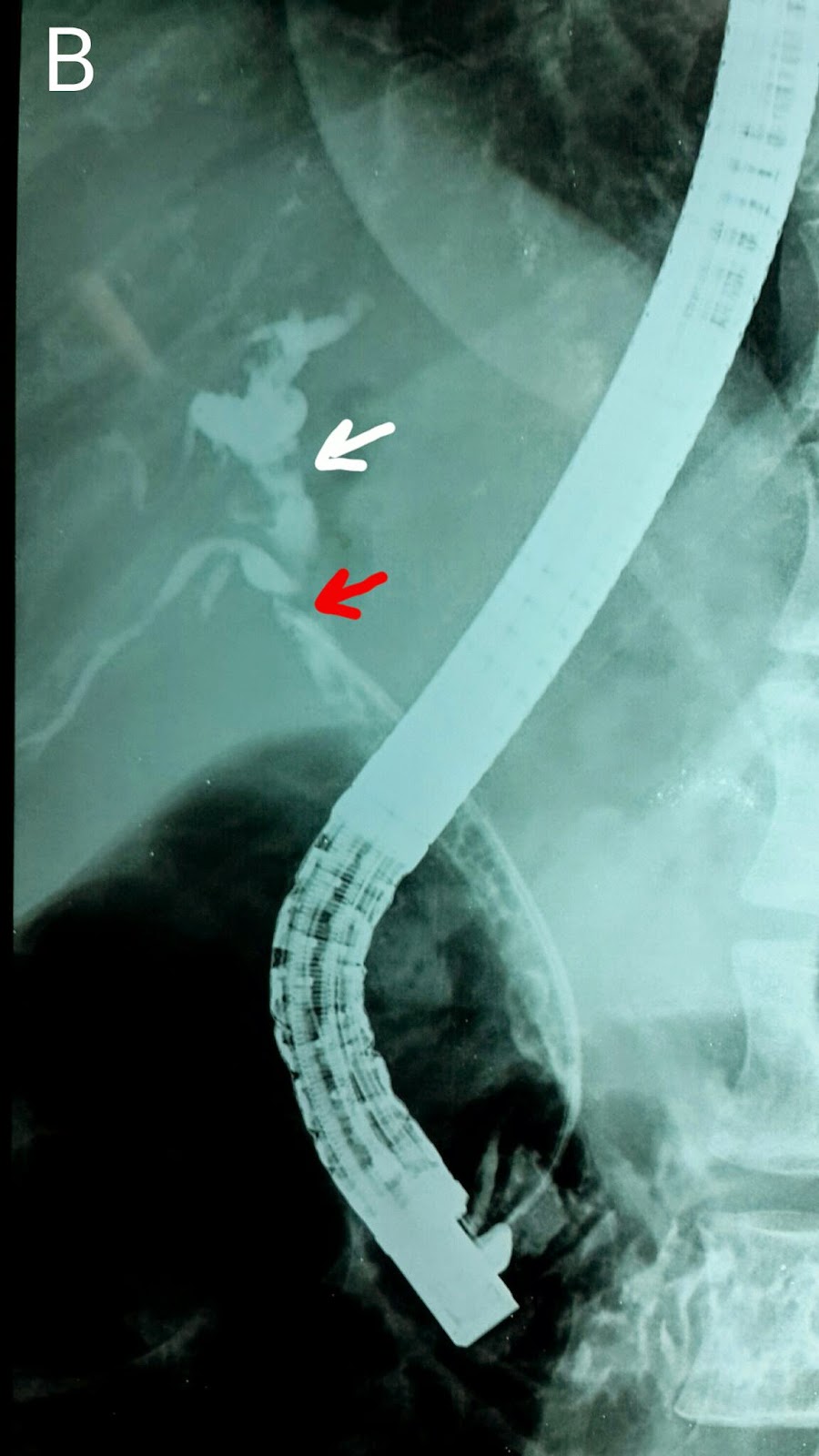
We last saw this 50 year old gentleman two and a half months earlier when we dilated his anastomotic stricture with a 6mm balloon and placed a 10 French stent http://ercp365.blogspot.com/2014/09/second-follow-up-ercp-for-post-liver.html. His bilirubin levels had started to rise and we expected a blocked stent. His ultrasound confirmed this with no pneumobilia. We removed his previous stent using a snare (A: White arrows mark the wires of the snare around the stent. Blue arrow marks the stent. A guidewire was manoeuvred across the stricture (B: Black arrow shows the level of the stricture on the guidewire). Contrast injection again confirmed the narrowing (C: Black arrows show the narrowing at the anastomotic site). We decided to go for a bigger balloon this time and an 8mm diameter balloon was placed across the stricture (D: White arrows). The balloon was inflated (E: White arrows show the inflated balloon with a "waist" formation at the specific point of concern). Following dilatation, repeat contrast injection showed adequate dilatation (F: Black arrows now show no narrowing). A stent assembly was then placed (G: White arrows). A 10 French plastic stent of 15 cm length was deployed.